Introduction:
Tunisia is a North-African, low-middle income country which had its independence in1956.
During the 1960s, the state directed development as described by WALT and GILSON (1), with a very important governments' role: free and compulsory education, development of a national health system with a strong provision of public services, adoption of a Beveridgien system (2) …
Following the independency, there has been demographic (population that tripled (3), life expectancy increased and infant mortality that declined (4) (5)) and epidemiological transitions (decline and even eradication of some transmissible diseases and a rise in the non-communicable diseases (3)).
Following the two oil crises (in 1973 (6) and in 1978 (7)), the government decided to start austerity reforms and tried implementing SAP[1]conditionalities which were poorly received by the population (8).
Despite the improvement in health indicators, there have been dramatic deterioration of living conditions and extending inequalities (1) that were associated with an “insurmountable” debt.
During the 1980s and 1990s, under the influence of “Internationally minded organizations” (Bollini and Reich. 1994), the country had to implement some neo-liberal reforms in the Healthcare system with a more market-oriented provision and gradually replaced the Beveridgien system by a predominantly Bismarckian one (2).
During this period, the gaps between the rich and the poor worsened and the level of unmet needs in healthcare increased. The overall healthcare system kept a normative notion of health care need (9) with a paternalistic approach going along with the biomedical model. There have been serious operational problems, affecting the availability, quality and safety of services. Public health facilities did not see much improvement and market-oriented policy led to a flourishing private sector localized only in advantaged areas.
In this article, we will try to describe the Tunisian health system, to assess its capacities, to analyze how it has adapted or not during the COVID-19 epidemic and to offer recommendations aiming the improvement of access to care in the context of the pandemic and for the upcoming years.
Health care system in Tunisia:
Tunisian Health system Framework:
The WHO framework (10) will be used to describe the organization of the Tunisian health system.
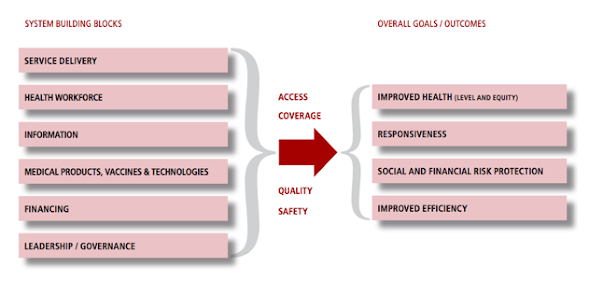
Figure 1: The WHO health system framework
Health services:
Healthcare provision’ organization has a traditional taxonomy (11). Public is state owned with some structures belonging to public non-state organizations (12). The private sector is made of an important majority of for-profit providers made of GP and specialists owned businesses as well as corporations. For-non-profit providers are a minority (NGOs).
The private sectoris rather flourishing but very unevenly distributed over the territory. It remains financially inaccessible for a vast majority of Tunisians.
The public sector is designed in 3 levels of care (12): Primary, secondary and tertiary.
Level | Category | Number of structures |
Tertiary | Public Health Establishments University hospital center | 21 |
Secondary | Specialized centers | 6 |
Secondary | Regional Hospitals | 33 |
Secondary | District Hospitals | 109 |
Primary | Basic Health Groups | 24 |
Primary | Basic Health Centers/ PHCs | 2058 |
Primary | Regional centers for school and university medicine | 9 |
University hospitals are located in areas of solvency. There is a lack of healthcare provision in second level structures located in rural and sub-rural areas.
PHC structures have a good territorial distributionbut provision of care is insufficient.
The public sector provides 2/3 of consultations and 90% of hospitalizations but has less funds than the private sector and a limited service package.
Preventive and promotional activities are marginalized with a very low budget (13).
Health workforce:
SAP inspired policies offering voluntary departure programs, early retirements and vulnerable contracts for health providers (14) seems to have accelerated the massive departure of doctors also justified by unfavorable working and living conditions (15).
Meanwhile, European countries have migration policies that promote qualified migration. Qualified migrants are paid less than Europeans for the same work, are poorly unionized and are assigned to positions where the workload is heavier. However, people migrate because there is still an improvement in their socio-economic status and better respect of their human rights.
On the other hand, many autochthone health providers have unregulateddual membership in both public and private sectors, opening the doors to corruption.
Health financing:
Public health expenditure was below 4% in 2017 and Health expenditure was around 7% during the past years.
There are 4 types of funds for the healthcare system (13) :
-34.6% Social insurance
-39.4% OOP payment (full payment, Co-payment and User fees)
-24.1% Taxation
-1.3% Private insurances
More than 80% of Tunisians have some coverage (16). The state guarantees free or subsidized health care to the lowest income groups (3).
The coverage rate is 100% for public sector workers and reaches 95% in the private sector and unemployed are excluded.
Equitable access:
National horizontal health programs are free. Access to other health services varies:
-Insured can choose public or private providers. Reimbursements are capped.
-Beneficiaries of free health care and reduced rates are entitled only to public providers.
Health information system:
Tunisian Health information system is evaluated by the WHO as being underdeveloped (17).
Leadership and governance:
The context is instable: there have been 5 health ministers during 2020.
Political responses were often reactive and neither met the needs, nor had prospects for lasting solutions.
Marked corporatism bogs an already complicated situation.
In addition to the structural governance problems, corruption seems to affect the various links of the chain.
The traditional and centralizing administrative burden does not allow an effective and adequate use of modern technologies, which intensifies the administrative compartmentalization, the lack of traceability and the lack of data.
In conclusion, many obstacles add up to the deficiencies in governance, management, regulation, financing and participation to make the health system inefficient and inequitable.
Barriers to access health services:
The main barrier is financial: poor people are entitled to public health structures that are underfunded and poorly managed, while the well-off have can chose the private sector, producing a Two-tier health system. In addition, corruption produces an added financial barrier since patients are facing money extortion in public structures in order to access services and might be directed to private sector with its financial implications.
The second barrier is structural: lack of specialists and medical technologies pushes patients to turn to university hospitals with all that this implies in terms of access difficulties and prolonged waiting times or again to private sector.
Performance of the healthcare system:
The WHO defines performance as the evaluation of the achievement of the objectives of a health system in comparison with “what it should be able to accomplish”if it was efficient (18).
Improving its own performance is one of the objectives of a health system. Performance assessment is based on the analysis of specific indicators considering various dimensions like effectiveness, fairness in financial contribution and responsiveness(19):
Effectiveness:
Indicators show that the Tunisian health system is insufficiently contributing to better health in the population.
Indicators | Year 2000 | Year 2017 |
MMR[2](per 100 000LB) (20) | 66 | 43 |
IMR[3](per 1 000 LB) (21) | 24.9 | 14.7 |
LEB[4](years) (4) | 73.1 | 76.3 |
MMR is relatively high (22) and noncommunicable diseases are the cause of more than 8 out of 10 premature deaths and contribute to more than 63% of current health expenditure in 2014 A recent study shows that six (6) in ten (10) hypertensive people are unaware of their situation today and only one (1) in four (4) diabetics are balanced(23).
We can conclude that the effectiveness of the Tunisian healthcare system isn’t satisfying.
Fairness in financial contribution:
Tunisia was ranked between 108 and 111 from a total of 191 countries according to the WHO report when it comes to fairness in financial contribution (24).
Indeed, though Kakwani index indicate a progressive healthcare financing system (25), the latter fails to have its redistributive role since the tax administration doesn’t work appropriately (16).
Protection against sickness is insufficient: 17% of the population isn’t covered and important OOP without any possibility of reimbursement, lead to pushing 100 thousand people into poverty every year.
Regional disparities are also significant: in disadvantaged areas, almost a third of the population (32.3%) have no social health coverage.
Responsiveness
Responsiveness has two major sections: the first is ‘‘respect for persons’’ including therespect of dignity, individual autonomy and confidentiality; the second is named ‘‘client orientation’’ and is about satisfaction (26).
According to WHO, Tunisia is ranked between 60 and 61 when it comes to the distribution of responsiveness (evaluating inequalities) and its health system level of responsiveness is the 94thamongst the total member-countries (27).
COVID-19 epidemic:
Tunisia faced a tremendous 4thwave in June 2021. The delta variant touched all the territory. Mortality rate due to COVID-19 was the highest in Africa (28).
.
The delta variant of the virus quickly gained ground to affect the vast majority of the territory. The daily cases reached more than 9 200 cases on daily basis, incidences were very high (the highest was 538.07 new infections /100,000 inhabitants/ 7 days on the 14/07/2021), testifying to the failure of measures taken to contain the spread of the epidemic.
New challenges plagued the healthcare system since therewas a “huge gap" (WHO 2021) between the needs and the resources available: the number of ICU beds was insufficient (29), there have been many shortages in Oxygen Supply… The situation was critical and the spokesperson for the ministry of health publicly announced the collapse of the health system (30).
The adaptation of health services provision during the COVID-19 epidemic had the theoretical objective of increasing the number of beds for potential patients in respiratory distress. There was a cancellation of all scheduled and routine activities. Sexual and reproductive health services have been seriously impacted with a significant decline in access for women: pregnancy follow-ups have been interrupted, some deliveries have taken place at home, family planning services have been completely interrupted.
The prioritization went hand in hand with the conservative anti-contraception and anti-abortion tendencies of the minister at the time (31).
Thanks to an international mobilization, provision of healthcare has been adapted through implementation of buffer hospitals and the vaccination program, but these adaptations happened when Reff was firmly inferior to 1(28).
The COVID-19 epidemic exposed the pre-existing failures of the Tunisian healthcare system.
Policy recommendations:
It is important to have comprehensive policies to ensure the protection of the health of the population.
There are barriers that doesn’t allow the Tunisian health system to evolve and upon which the state needs to act:
-Regulation of the entire health sector including public and private sectors in order to fight corruption should be a priority. Several elements combine to make the health system prone to corruption in order to establish the principle of accountability to the population served.
On a practical level, the computerization of management systems and patient records would allow traceability and thus impose transparency by making reliable, available and usable information on the nature of the services and the conditions of their use over time and in the space.
-The adaptation of regulations and laws in the health sector is necessary in order to give health authorities the mandate and the means to regulate the entire health sector, public and private. This regulation should have as a priority the reduction of direct household expenditure and the extension of health coverage to the entire population without exclusion, by guaranteeing a package of essential services provided in a complementary manner by the public and private sectors.
Once the effect of the barriers to change begins to wear off, a health system performance enhancement can really take place.
Stakeholders must assume their responsibilities in the promotion and protection of health. It is therefore necessary to increase the budget allocated to health but also to take health into account in economic, environmental and development policies.
Conclusion:
Health is a human right; it is also a constitutional right. Health cannot be thought of and managed through a market-oriented approach.
Until now the health sector has been managed as a department in charge only of diseases and hospitals. This constitutes a bias which has done a lot of harm. Protection and promotion of health must be a transversal concern of all sectors.
The current crisis should serve as an opportunity for the implementation of a patient-oriented health system with an effective consideration of health protection as well as the consideration of equity, solidarity and quality in access to services.
References:
1. WALT G, GILSON L. Reforming the health sector in developing countries: the central role of policy analysis. Health Policy and Planning. 1994;9(4):353-370.
2. Republic of Tunisia Health sector study [Internet]. Documents1.worldbank.org. 2006 [cited 22 October 2021]. Available from: https://documents1.worldbank.org/curated/en/201241468312891649/pdf/410180ENGLISH010Sector0Study10Final.pdf
3. Achour N. LE SYSTEME DE SANTE TUNISIEN : « ETAT DES LIEUX ET DEFIS » [Internet]. Fphm.rnu.tn. 2011 [cited 22 October 2021]. Available from: http://www.fphm.rnu.tn/sites/default/files/Annexe%202%20Le%20système%20de%20santé%20tunisien%202011%20Noureddine%20Achour.pdf
4. Life expectancy at birth, total (years) - Tunisia | Data [Internet]. Data.worldbank.org. 2021 [cited 22 October 2021]. Available from: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=TN`
5. Anonymous NIS/UNICEF (2013) Situation des enfants et des femmes en Tunisie – Enquête par grappes à indicateurs multiples 2011–2012. Available: http://www.ins.nat.tn/. Accessed 31 July 2013.
6. Corbett. Oil Shock of 1973–74 | Federal Reserve History [Internet]. Federalreservehistory.org. 2021 [cited 15 November 2021]. Available from: https://www.federalreservehistory.org/essays/oil-shock-of-1973-74
7. Graefe. Oil Shock of 1978–79 | Federal Reserve History [Internet]. Federalreservehistory.org. 2021 [cited 15 November 2021]. Available from: https://www.federalreservehistory.org/essays/oil-shock-of-1978-79
8. Houpert P. Le 29 décembre 1983, les émeutes du pain embrasent la Tunisie – Jeune Afrique [Internet]. JeuneAfrique.com. 2021 [cited 15 November 2021]. Available from: https://www.jeuneafrique.com/386581/politique/jour-2729-decembre-1983-debut-emeutes-pain-tunisie/
9. Harrison J, Young J, Butow P, Solomon M. Needs in Health Care: What Beast is That?. International Journal of Health Services. 2013;43(3):567-585.
10. EVERYBODY’S BUSINESS STRENGTHENING HEALTH SYSTEMS TO IMPROVE HEALTH OUTCOMES WHO’S FRAMEWORK FOR ACTION [Internet]. Apps.who.int. 2007 [cited 15 November 2021]. Available from: https://apps.who.int/iris/bitstream/handle/10665/43918/9789241596077_eng.pdf
11. Saltman R. Melting public-private boundaries in European health systems. The European Journal of Public Health. 2003;13(1):24-29.
12. Structures publiques de santé en tunisie - Ministère de la santé publique [Internet]. Santetunisie.rns.tn. 2021 [cited 15 November 2021]. Available from: http://www.santetunisie.rns.tn/fr/carte-sanitaire/structures-publiques-de-sante-en-tunisie
13. Ben Abdelaziz A, HAJ AMOR S, Ayadi I, Khelil M, Zoghlami C, Ben Abdelfattah S. Article medicale Tunisie, Article medicale Financement des soins de santé - Dépenses de santé - Participation aux coûts- Financement du gouvernement - Financement individuel - Soutien financier à la planification et au développement de la santé - Assurance maladie - Couverture d'assurance - [Internet]. Latunisiemedicale.com. 2018 [cited 21 October 2021]. Available from: https://www.latunisiemedicale.com/m/article-medicale-tunisie_3467_fr
14. Le FMI se dit prêt à accompagner la Tunisie dans ses réformes économiques [Internet]. Le Monde.fr. 2021 [cited 30 June 2021]. Available from: https://www.lemonde.fr/afrique/article/2021/05/07/le-fmi-se-dit-pret-a-accompagner-la-tunisie-dans-ses-reformes-economiques_6079444_3212.html
15. Les intentions et motifs d'émigration des jeunes médecins de famille, objet d'une thèse de doctorat en médecine [Internet]. Leaders. 2021 [cited 30 June 2021]. Available from: https://www.leaders.com.tn/article/31499-les-intentions-et-motifs-d-emigration-des-jeunes-medecins-de-famille-etude-realisee-dans-le-cadre-d-une-these-en-medecine
16. Boughzala M, El Lagha A, Bouassida I, Ferjani M. Les inégalités en Tunisie [Internet]. cairn.ifo. 2020 [cited 15 November 2021].Available from: https://www.cairn.info/papiers-de-recherche--1000000148925-page-1.htm
17. Health profile 2015: Tunisia [Internet]. Apps.who.int. 2021 [cited 15 November 2021]. Available from: https://apps.who.int/iris/bitstream/handle/10665/254904/EMROPUB_2017_EN_19615.pdf
18. Health systems: improving performance. Geneva: WHO; 2000.
19. MEASURING UP: IMPROVING HEALTH SYSTEM PERFORMANCE IN OECD COUNTRIES. PARIS 2 RUE ANDRE PASCAL: OECD; 2002.
20. Maternal mortality ratio (modeled estimate, per 100,000 live births) - Tunisia | Data [Internet]. Data.worldbank.org. 2021 [cited 16 November 2021]. Available from: https://data.worldbank.org/indicator/SH.STA.MMRT?locations=TN
21. Mortality rate, infant (per 1,000 live births) - Tunisia | Data [Internet]. Data.worldbank.org. 2021 [cited 16 November 2021]. Available from: https://data.worldbank.org/indicator/SP.DYN.IMRT.IN?locations=TN
22. Tej Dallagi R, Bougatef S, Ben Salah F, Ben Mansour N, Gzara A, Gritli I et al. National survey of maternal mortality in 2010: data of Tunis [Internet]. Applications.emro.who.int. 2021 [cited 16 November 2021]. Available from: https://applications.emro.who.int/imemrf/Tunisie_Med/Tunisie_Med_2014_92_8_9_560_566.pdf
23. Saidi O, Zoghlami N, Aounallah-Skhiri H, Skhiri A, Ben Mansour N, Hsairi M. La santé des Tunisiens Résultats de l’enquête «Tunisian Health Examination Survey-2016» [Internet]. Santetunisie.rns.tn. 2019 [cited 16 November 2021]. Available from: http://www.santetunisie.rns.tn/images/rapport-final-enquete2020.pdf
24. The World health report 2000 Health systems: improving performance. Geneva; 2000
25. Rostampour M, Nosratnejad S. A Systematic Review of Equity in Healthcare Financing in Low- and Middle-Income Countries. Value in Health Regional Issues. 2020;21:133-140.
26. Murray C, Frenk J. A framework for assessing the performance of health systems [Internet]. PubMed. 2021 [cited 17 November 2021]. Available from: https://pubmed.ncbi.nlm.nih.gov/10916909/
27. Valentine N, De Silva A, Murray C. Estimating Responsiveness Level and Distribution for 191 Countries: Methods and Results [Internet]. Citeseerx.ist.psu.edu. 2000 [cited 17 November 2021]. Available from: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.172.2124&rep=rep1&type=pdf
28. Tunisia COVID-19 report [Internet]. Mrc-ide.github.io. 2021 [cited 18 November 2021]. Available from: https://mrc-ide.github.io/global-lmic-reports/TUN/
29. Marbot O. Nombre de lits de réanimation et de respirateurs : où en est l’Afrique ? – Jeune Afrique [Internet]. JeuneAfrique.com. 2021 [cited 17 November 2021]. Available from: https://www.jeuneafrique.com/924087/societe/nombre-de-lits-de-reanimation-et-de-respirateurs-ou-en-est-lafrique/
30. Tunisia says health care system collapsing due to COVID-19 [Internet]. Reuters. 2021 [cited 17 November 2021]. Available from: https://www.reuters.com/business/healthcare-pharmaceuticals/tunisia-says-health-care-system-collapsing-due-covid-19-2021-07-08/
31. Dahmani F. Tunisie : l’accès des femmes à la santé, victime collatérale du Covid-19 – Jeune Afrique [Internet]. JeuneAfrique.com. 2021 [cited 18 November 2021]. Available from: https://www.jeuneafrique.com/986012/societe/tunisie-acces-des-femmes-a-la-sante-victime-collaterale-du-covid-19/
Aucun commentaire:
Enregistrer un commentaire