In this article, I offer an analysis of the epidemiological data about the management of the COVID-19 epidemic from its beginning until July 2021 in Tunisia.
I go through the different determinants in relation to the severity of this epidemic in Tunisia and comment on the availability, quality and relevance of the epidemiological data available.
Introduction
Tunisia has been dealing with Covid-9 cases since the end of July 2020. It had been fairing ok for some times in terms of overall management and at times, referred to as having a “successful response”.
There were peak incidences of cases from July to November 2020, from December 2020 to end of February 2021, from April to mid-May 2021 and finally a steady climbing of cases from end of May with an acceleration of cases in June 2021 (1).
The daily cases peaked at most to around 5000 daily cases for the first three peaks but since the second week of July, it reached more than 9 200 cases on a daily basis (1).
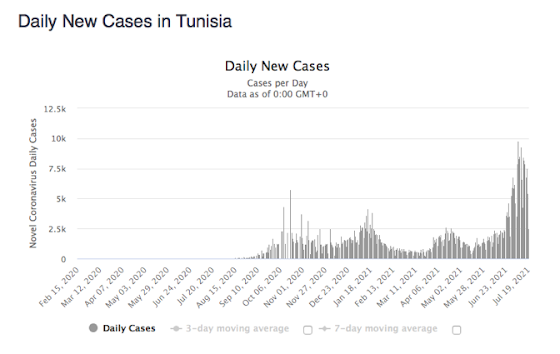
Figure 1: Daily New cases of COVID-19 infection in Tunisia
Source: Worldometers
Trends across time (2):
Maps elaborated by ONMNE[1]show the variability and the evolution of the level the incidence every 14 days, by governorate and by delegation in the country between 21stof September until the 4thof January 2021.
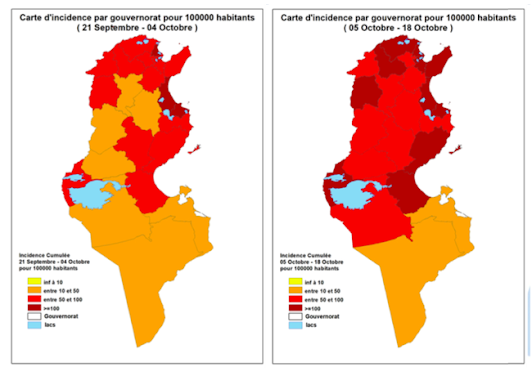
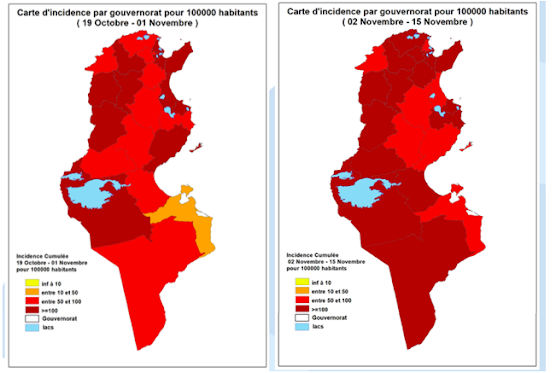
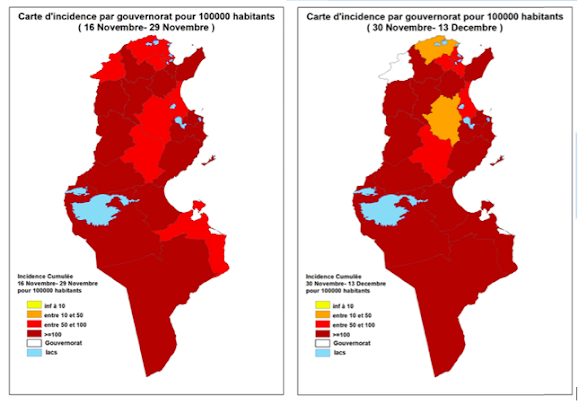
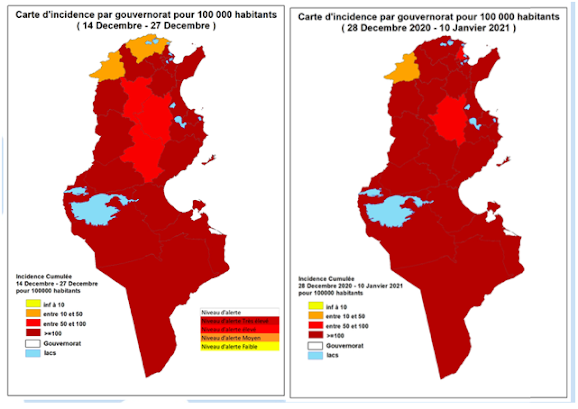
Figure 2 : Variability and evolution of the level of risk by governorate between 21 september 2020 until 10 january 2021
Source: OMNE / COVID-19 en Tunisie Bulletin de veille Published on the 15 Janvier 2021(2)
The virus continued to progress and quickly gained ground to affect the vast majority of regions in Tunisia, reaching incidences of more than 100 per 100,000 inhabitants per 14 days over almost the entire country, testifying to the failure of measures taken to contain the spread of the epidemic in Tunisia.
It is also interesting to compare incidence of COVID-19 infection during the highest peaks of transmission with other countries. As shown in the table, Tunisia has higher incidence than Brazil and India when having the highest peak of transmission (3).
Country | Date of the highest peak of transmission | Incidence of new infections /100,000 inhabitants/ 7 days |
Tunisia | 14/07/2021 | 538.07 |
Brazil | 26/06/2021 | 338,15 |
India | 08/05/2021 | 283,50 |
USA | 10/01/2021 | 743,48 |
France | 05/11/2020 | 679,03 |
Table1: Comparing the highest incidences of new cases of COVID-19 infection per 100,000 inhabitants per 7 days in Tunisia, Brazil, India, USA and France
Source: Our World in data
Distribution:
On the 19thJuly 2021, total number of cases reported by Worldometers (1) was 548,753, of which 438,356 are considered recovered, 92,753 are active and 17, 644 are confirmed deaths.
At the national level, the lethality (per 100 COVID-19 cases detected) was 3.3%, it varied from 6.8% in Jendouba (rural deprived area) to 2.9% in Touzeur (2).
INS[2]report(4)shows that Mortality ratehas increased in 2020, in Tunisia by 5.3%. Deaths recorded during the first 6 months of 2021 were nearly the double all deaths in the year 2020, including the increase observed during the year 2020 due to mortality induced by COVID-19 (5).
Demographic factors (2):
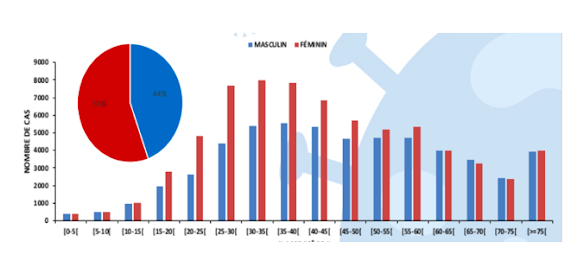
Figure 3: Distribution by Sex and Age until January 2021
Source: OMNE / COVID-19 en Tunisie Bulletin de veille Published on the 15 Janvier 2021(2)
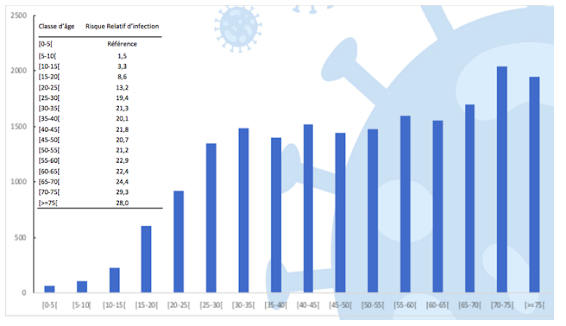
Figure 4: Incidence by age until January 2021
Source: OMNE / COVID-19 en Tunisie Bulletin de veille Published on the 15 Janvier 2021(2)
The incidence rate was higher in females for those aged 15-60 (in subjects aged between 15 to 60 years, 56% of the positive cases reported by ONMNE were female), comparable between the two genders for those under 15 and 60-65 and higher in males for those aged 65 and over. (Figure 3)
Subjects under 20 years of age accounted for 6.8% of confirmed cases, those aged 20 to 60 years 71.2% and those over 60 years 22.0%. (Figure 3)
The incidence rate (per 100,000 inhabitants) of confirmed cases was between 69.6 and 601.5 in people aged under 20. (Figure 4)
This incidence rate was multiplied by 20 and even 30 for the other age groups compared to children under 5. (Figure 4)
Determinants of COVID 19 infection and mortality
Individual Risk factors:
Age:
Statistics in Tunisia confirm that older age(6) is a risk factor for developing a severe COVID-19 infection as shown in Figure 4. Indeed, the median age of the deceased was 72 years (63-81 years). Over 80% of deceased COVID-19 cases were aged 60 or older as shown in figure 5.
The ONME report (2) mentions that mortality rate was highest for subjects over 75 years old: taking the 45-50 age group as a reference, the death rate was multiplied by 38 for subjects over 75 years old, 22 for 70-74 year old, 18 for 65-69 year old, 9 for 60-64 year old, 4 for 55-60 year old and 2 for 50-54 year old.
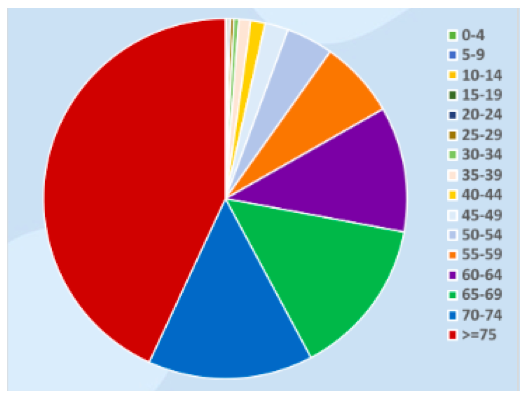
Figure 5: Deaths due to COVID 19 in Tunisia by age until January 2021
Source : OMNE / COVID-19 en Tunisie Bulletin de veille Published on the 15 Janvier 2021(2)
Gender:
Although COVID infection incidence was higher in females (56% versus 44% in males), there has been a more important death rate in Males. Genderbeing a risk factor for severe COVID infection (men being more prone to develop an infection (7)) has been also confirmed since, the Male / Female sex ratio of deaths was 1.9 with 66% of deaths in male.
Comorbidities:
Comorbidities are known to be a determinant for severe COVID cases: diabetes (6), hypertension (8), cardiovascular disease(8), malignancy (9) and other health issues like : obstructive and restrictive pulmonary disease, chronic renal disease, malnutrition, immunodeciency and autoimmune diseases, high body mass index (BMI), stress …(10)
A descriptive study (11) about 20 hospitalized patients in Tunisia, report 80% with at least one comorbidity.
One might think that people already infected with COVID-19 and having pulmonary sequels could be more at risk of developing severe to deadly infections if they are infected (12). Given the lack of receipt, there have not yet been studies on the 2nd infections and their impact.
Environmental risk factors
Rural Areas:
Having a weak health systemseems to be a very important risk to deadly COVID infection. Indeed, the actual health model was built after the independence and has not changed since though Tunisia's demographic situation has evolved: population tripled since 1960, life expectancy increased… This demographic and epidemiological transition (13) had consequences to which the health system failed to adapt.
The fragmented and complex health insurance system is inequitable and generates corruption, making access to health care unfair: nearly 2 millions Tunisians have no social health coverage (14) and those affiliated to health protection system don’t access equal services: poor people are entitled to public health structures that are underfunded and poorly managed, while the well-off have can chose the private sector.
In addition, there are huge disparities in health services availability between rich areas and less lucky ones and we can see the impact of this unfair health system through COVID mortality: the highest mortality rates due to COVID-19 by region (per 100,000 inhabitants) were observed in areas with insufficient health system like Kébilli (85.2) and Tataouine (76.0) until January 2021. After that clusters continued to appear and there are epicentres of COVID 19 cases in other deprived areas like Beja and Siliana governorates.
In these rural areas, contact with animalslike cat, dog, cattle and sheep (15) could be also a determinant in high transmission of COVID 19, but there has been no reported testing in animals.
Urban areas:
The capital kept registering one of the highest mortality rates since the beginning of the pandemic(around 67.3 per 100,000 inhabitants).
Greater Tunis is an urban area that represent 2% of the country's surface and counts 23% of the national population (16). It is one of the most crowded areas in the country, which consists a determinant for COVID-19 infection (17). In addition, informal settlements are frequent in the areas surrounding the Greater Tunis and are due to internal migration. They are characterized by a poor population rejected on the outskirts of the city and marginalized. This destitute population has few resources. It is excluded from the formal housing sector because of their limited means, their lack of access to housing finance systems, and the insufficient production of social housing or its high cost. This is housing that is often not connected to the sanitation system (18). Bad water and sanitation system, through infected human feces represent an environmental risk for COVID-19 (19) and probably contribute to this continuous high mortality rate in Tunis.
Other risk factors:
There are other environmental and community risk factors that haven’t been studied in Tunisia like:
-Low education (20)
-Occupational risks
-Poor ventilation (21)
-Other environmental factors including living conditions, unemployment (10) and incidence of infection in closed settings like prisons.
-vulnerable migrant population with low access to health services
Viral risk factors
The mutationsof the virus produce variants with different virulence, replication, higher transmission (delta variant), various immune responses…
These changes in the virus structure might produce variants with higher risks for younger people.There seems to be no systemic screening of sample for variants of concern.
On the other hand, while the virus load in asymptomatic and symptomatic patient was reported to be similar, some studies show a more important production of virus in asymptomatic individuals leading to greater transmission if protective measures aren’t respected (21).
Collection of Epidemiological data
The challenge of Data collection:
Like in other contexts, data collection doesn’t seem to be complete and systematic (22). Unlike the USA where the reporting of the possible and confirmed cases is done by hospitals, healthcare providers, and laboratories, in Tunisia, only confirmed cases of COVID-19 were reported to ONMNE by the network of public laboratories (2).
Private laboratories and doctors in the private sector seem to be underreporting. The causes might be various (23).
The data is first consolidated by regional units then by ONMNE unit (2). There have been delays in data consolidation and an incomplete integration of confirmed cases in the "SARS-CoV-2" database.
The actual number of confirmed cases is also probably underestimated due to the lack of systematic screening of symptomatic or asymptomatic infected people and a relatively low targeted screening rate in Tunisia.
Deaths liked to COVID appear to happen in majority in the hospital. Only 12% are reported to take place outside the hospital (24).
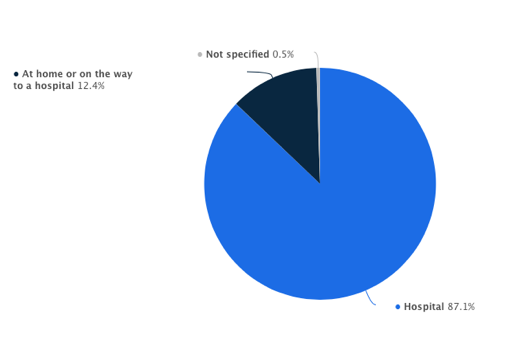
Figure 6 : Distribution of coronavirus (COVID-19) deaths in Tunisia as of January 2021, by place of death
Source: Statista
There seems to be also a bias in data collection about deaths, since it has been reported that many families prefer to keep their elderly at home even if they are sick because they are afraid that they will not be able to perform the burial rituals properly due to restrictions in handling the bodies of those who have died from COVID.
Different definitions and different data:
There are no instant official data available about COVID in Tunisia, but many websites are publishing data that is collected from several sources.
National sources:
· Tunisian Ministry of Health: https://www.facebook.com/santetunisie.rns.tn/
· Observatoire National des Maladie Émergentes (National Observatory for Emerging Diseases) : https://www.onmne.tn
· EVAX for vaccination : https://www.evax.tn
· Institut National des Statistiques (National institute of statistics): http://www.ins.tn
International sources:
- World Health Organization (WHO): https://covid19.who.int/region/emro/country/tn
Media:
- WorldoMeters: https://www.worldometers.info/coronavirus/
- Our World in Data : https://ourworldindata.org/search?q=Tunisia+covi
- COVID RADAR 24: https://www.covidradar24.org/web/dhafer.malouche/home
- CORONAVIR: https://www.coronavir.org/data/tunisie
- Reuters : https://graphics.reuters.com/world-coronavirus-tracker-and-maps/fr/countries-and-territories/tunisia
- CORONATRACKER : https://www.coronatracker.com/fr/country/tunisia
- STATISTA: https://www.statista.com/statistics/1110895/coronavirus-cases-in-tunisia/
- INKYFADA: https://inkyfada.com/en/2021/02/26/dashboard-covid-19/
Media are mainly using secondary data and definitions adopted to collect data seem to vary. For example, Worldometer follows the new CDC guidelines (25), that define total death cases as the total of confirmed cases and probable cases. On the other hand, Reuters follow the WHO recommendations (26): counting methods do not include undiagnosed cases and deaths (27). These differences in the definitions lead to different data depending on the source.
For example, for the 20 July 2021, these two medias presented different statistics:
MEDIA | TOTAL CASES | TOTAL DEATHS |
WORLDOMETER (1) | 548 753 | 17 644 |
REUTERS (27) | 546 233 | 17 527 |
Table 2: total number of COVID cases and total number of COVID related deaths reported in the two websites Wordldometer and Reuters on the 20thJuly 2021
In addition, the presentation of the data is not harmonized, in fact the incidence is presented with different measurements and parameters, the means do not describe the same periods ... which can cause confusion.
Application of epidemiological knowledge to public health practice and knowledge:
There was never a strategy of covid19 zero and the lowest incidence of cases since the July 2020 went to few hundreds of cases per day. Hence, brewing “under the radar” community transmission had been let to happen.
Indeed, the current peak of cases is not fully explained but we can imagine that by the end of Ramadan (mid-April) with laxity on public health measure, summer months with indoor living under air conditioning, may be greater access to testing and possibly the introduction of other variants of concern, including the Delta one might have led to this situation.
At the national level:
The overarching strategy of the Ministry of Health to decongest the public hospitals are to generate more hospital beds through the creation of “Hôpital de campagne/Hôpital de circonstance”. There is a plan of 9 of those buffer hospitals across the country. Those buffer hospitals have been set up in sports building (gymnasiums). The key issue about those structures is to operationalize them through right staffing and medical supply namely in terms of O2 but as well monitoring and treatment (re: low weight heparin).
At the international level:
Faced with the alarming figures, there was a great mobilization of the international community: many countries have started to donate medical equipment, oxygen, vaccines ...
International organizations such as Doctors without Borders have also rallied to help the Ministry of Health in the fight against the epidemic.
Conclusion and Recommendations:
Tunisia is facing a critical situation during this COVID-19 pandemic which is affecting a very fragile health system. the reported incidence is very high, the lethality rate is high since the health system is inefficient and the unstable political situation does not allow the success of restrictive movement measures.
Government decisions as well as international decisions to classify the country in the red zone are based on the observation of the pandemic trends in the country.
Completeness, accuracy and timely flow of data are crucial to evaluate the importance of the impact of the COVID -19 pandemic in population.
Data collection and analysis need to be timely effective in order to help take efficient decisions, but this is also a great challenge since sources of data are very various and definitions aren’t standardized.
There is a need for more centralized, rapid and effective official communication of reliable data by the Ministry of Health in Tunisia.
References
1- Tunisia COVID: 554,911 Cases and 17,821 Deaths - Worldometer [Internet]. Worldometers.info. 2021 [cited 19 July 2021]. Available from: https://www.worldometers.info/coronavirus/country/tunisia/
2- Hechaichi A, Letaif H, Safer M, Dhaouadi S, Osman M, Ben Salah H. Bulletin COVID-19 en Tunisie: Bulletin de veille -15 Janvier 2021 [Internet]. Onmne.tn. 2021 [cited 20 July 2021]. Available from: https://onmne.tn/wp-content/uploads/2021/01/bulletin-COVID-19-du-15-Janvier-2021-NBA.pdf
3- Ritchie H, Ortiz-Ospina E, Beltekian D, Mathieu E, Hasell J, Macdonald B et al. Coronavirus Pandemic (COVID-19) [Internet]. Our World in Data. 2021 [cited 21 July 2021]. Available from: https://ourworldindata.org/coronavirus/country/tunisia
4- Dynamique récente de la mortalité en Tunisie [Internet]. Ins.tn. 2021 [cited 20 July 2021]. Available from: http://www.ins.tn/sites/default/files/publication/pdf/Mortalité_2020.pdf
5- The COVID-19 Epidemic in Tunisia, in Numbers [Internet]. Inkyfada. 2021 [cited 21 July 2021]. Available from: https://inkyfada.com/en/2021/02/26/dashboard-covid-19/
6- Zhou F. Clinical Course And Risk Factors For Mortality Of Adult In Patients With COVID-19 In Wuhan, China: A Retrospective Cohort Study. Journal of Medicine Study & Research. 2020;3(1):01-02.
7- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet. 2020;395(10223):507-513.
8- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA. 2020;323(11):1061.
9- Liang W, Guan W, Chen R, Wang W, Li J, Xu K et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. The Lancet Oncology. 2020;21(3):335-337.
10-Rashedi J, Mahdavi Poor B, Asgharzadeh V, Pourostadi M, Samadi Kafil H, Vegari A et al. Risk Factors for COVID-19 [Internet]. Infezmed.it. 2021 [cited 21 July 2021]. Available from: https://www.infezmed.it/media/journal/Vol_28_4_2020_2.pdf
11-Louhaichi S, Allouche A, Baili H, Jrad S, Radhouani A, Greb D et al. Caractéristiques des patients hospitalisés en pneumologie pour une infection COVID-19 : Première série Tunisienne [Internet]. Latunisiemedicale.com. 2021 [cited 21 July 2021]. Available from: https://www.latunisiemedicale.com/article-medicale-tunisie_3695_fr
12-Pachetti M, Marini B, Benedetti F, et al. Emerg- ing SARS-CoV-2 mutation hot spots include anovel RNA-dependent-RNA polymerase variant. J Transl Med. 2020; 18 (1), 179.
13- Wilkinson R, Pickett K. Spirit level. London: Penguin Books Ltd; 2011.
14- Rapport Sur Le Droit A La Santé En Tunisie Par L’Association Tunisienne de la Défense de Droit à la Santé [Internet]. Ftdes.net. 2021 [cited 30 June 2021]. Available from: https://ftdes.net/rapports/ATDDS.pdf
15- Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: impli- cations for virus origins and receptor binding. Lancet. 2020; 395 (10224), 565-74.
16-Tunis [Internet]. Marges & Villes. 2021 [cited 21 July 2021]. Available from: https://marges.hypotheses.org/valorisation/profils-de-villes/tunis
17- Wang P, Lu J, Jin Y, Zhu M, Wang L, Chen S. Statis- tical and network analysis of 1212 COVID-19 patients in Henan, China. Int J Infect Dis. 2020; 95, 391-8.
18-SOUISSI Ben HAMAD H. L’habitat informel en Tunisie : stratégies et orientations politiques [Internet]. Knowledgejournals.com. 2021 [cited 21 July 2021]. Available from: http://www.knowledgejournals.com/PDF/197.pdf
19- Sohrabi C, Alsa Z, O’Neill N, et al. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020; 76, 71-6.
20- Van Doremalen N, Bushmaker T, Morris DH, Hol- brook MG, Gamble A, Williamson BN, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020; 382 (16), 1564-7.
21- Lai C-C, Liu YH, Wang C-Y, et al. Asymptomatic carrier state, acute respiratory disease, and pneumo- nia due to severe acute respiratory syndrome coro- navirus 2 (SARSCoV-2): Facts and myths. J Microbiol Immunol Infect. 2020; 53 (3), 404-12.
22-Principles of Epidemiology: Lesson 5, Appendix E|Self-Study Course SS1978|CDC [Internet]. Cdc.gov. 2021 [cited 21 July 2021]. Available from: https://www.cdc.gov/csels/dsepd/ss1978/lesson5/appendixe.html
23- Marier R. The reporting of communicable diseases. Am J Epidemiol 1977;105:587–90
24-Tunisia: new daily coronavirus cases 2020-2021 | Statista [Internet]. Statista. 2021 [cited 21 July 2021]. Available from: https://www.statista.com/statistics/1110895/coronavirus-cases-in-tunisia/
25-COVID Data Tracker [Internet]. Centers for Disease Control and Prevention. 2021 [cited 21 July 2021]. Available from: https://covid.cdc.gov/covid-data-tracker/?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fcases-updates%2Fcases-in-us.html#cases_casesper100klast7days
26-Estimation de la mortalité due à la COVID-19 Document d’information scientifique 4 août 2020 [Internet]. Apps.who.int. 2021 [cited 21 July 2021]. Available from: https://apps.who.int/iris/bitstream/handle/10665/333842/WHO-2019-nCoV-Sci_Brief-Mortality-2020.1-fre.pdf
27-Tunisie: Les derniers chiffres, graphiques et cartes sur l'épidémie de COVID-19 [Internet]. Reuters. 2021 [cited 21 July 2021]. Available from: https://graphics.reuters.com/world-coronavirus-tracker-and-maps/fr/countries-and-territories/tunisia/
Aucun commentaire:
Enregistrer un commentaire